

The Staggering Scale of Trump’s 'War on HIV'
Mathematical models indicate that the worst-case scenario of the Trump administration's HIV-related cuts could result in 3 million deaths and an infection rate outpacing the virus’s peak in the 1990s.


Since 1989, the LGBT Life Center in Norfolk, VA has built up what CEO Stacie Walls calls a “test and treat” model. For every patient that walked through the doors of their HIV clinic after working up the courage to get tested, there had been the promise that, if they tested positive, all they’d need to do to get treatment is walk down the hallway.
But since the Trump administration’s sweeping cuts to HIV funding took place earlier this year, that’s no longer the case. “The grant money that pays for people who are uninsured is the grant money that they have canceled,” Walls told Uncloseted Media. “That’s so disheartening and scary and goes against everything that we’ve ever wanted to embrace as a nonprofit service agency.”
With these cuts, staff now have to send uninsured patients to the next nearest community HIV program in Hampton, a 30-minute drive away. Walls says they’ve already had to transfer 19 existing patients, including some of their frequent client base of low-income LGBTQ people of color, who are disproportionately impacted by the virus. While the center has been able to shift to covering at least their initial treatment appointment, they are unable to cover further care, and Walls says that even this is not sustainable.

The LGBT Life Center is just one of the many U.S.-based HIV organizations and programs that have fallen victim to the billions of dollars worth of cuts by Trump and his newly created Department of Government Efficiency.
HIV funding has been hit particularly hard: Uncloseted Media estimates that the National Institutes of Health (NIH) has terminated more than $1 billion worth of grants to HIV-related research.1 In addition, the U.S. Agency for International Development (USAID) has terminated 71% of all global HIV grants, and the President’s Emergency Plan for AIDS Relief (PEPFAR) has been the subject of temporary suspension and major proposed cuts.
Additional cuts are also on the horizon, with the Trump administration’s budget proposal for Fiscal Year (FY) 2026 calling for the closure of all Centers for Disease Control and Prevention (CDC) HIV programs.
The effects of these cuts are deadly. Researchers estimate that PEPFAR’s funding freeze alone may already be associated with more than 60,000 deaths in sub-Saharan Africa, and numerous experts say that the entire global health system could be upended if the administration's HIV cuts continue as planned. Mathematical models show that the worst-case scenario is apocalyptic: nearly 11 million new infections, 3 million deaths, and an infection rate outpacing the virus’s peak in the 1990s.
“This is not something that’s just a matter of the scientists losing funding; the community is losing funding, and in the long term, losing ground in the fight against HIV,” says Noam Ross, executive director at research nonprofit rOpenSci.
The Domestic Impact
Cuts to HIV funding in the U.S. have been a significant casualty of the Trump administration’s efforts to reduce spending and attack Diversity, Equity and Inclusion (DEI). Researchers behind Grant Watch, an independent third-party database of grants terminated by the NIH and the National Science Foundation, have identified HIV-related funding as one of the most common targets for termination. As of June 17, Uncloseted Media has calculated roughly $1.353 billion in HIV-related terminations in Grant Watch’s NIH database, accounting for more than a third of the $3.7 billion in recorded NIH cuts overall.
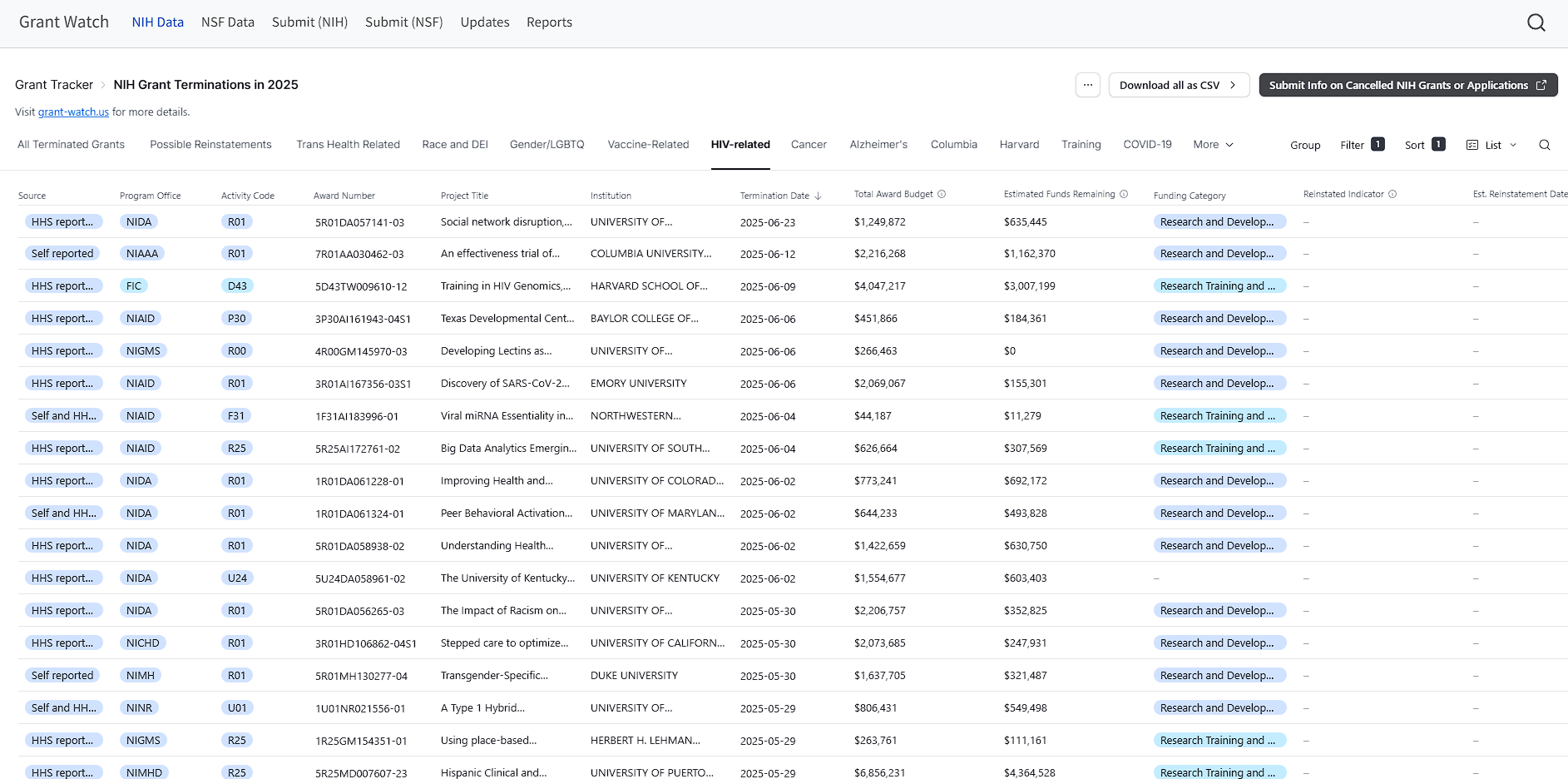
“They’re certainly casting an enormously wide net in this,” says Ross, who is also Grant Watch’s co-developer. “It doesn’t matter that they’re not explicitly saying that ‘it’s a war on HIV’ because if they’re gonna have a war on sexual minorities and transgender people, it’s a war on HIV too.”
The Department of Health and Human Services (HHS) has explicitly told HIV groups across the country that funding was cut because they believe health research for LGBTQ people and racial minorities is unscientific. Researchers across the country have received letters and emails from the NIH with nearly identical statements informing them of their grant terminations:
“Research programs based primarily on artificial and non-scientific categories, including amorphous equity objectives, are antithetical to the scientific inquiry, do nothing to expand our knowledge of living systems, provide low returns on investment, and ultimately do not enhance health, lengthen life, or reduce illness.”
One of the programs subjected to cuts is the Adolescent Medicine Trials Network (ATN), an HIV program that has been active since 2001. Its goal is to prevent, diagnose and treat HIV in young people.
Research under ATN’s umbrella has seen promising developments, including progress towards a product that could combine PrEP and birth control into one pill as well as new methods for reducing HIV transmission in young men who use stimulants. Despite this, NIH cut $15 million worth of grants to ATN because of its focus on high-risk LGBTQ youth populations. The program’s funds were later restored, but only after ATN agreed to cut off a study on transgender youth of color.
“There are particular issues around Black women, LGBTQ people, [and] the type of treatment that they need … that’s the social side of medicine, which is a very important part of medicine—it’s not just molecules, it’s people,” Ross says, adding that grantees focused on “delivery and participation and how to keep people in care,” such as programs that help vulnerable populations stay on PrEP or undetectable folks maintain their antiretroviral therapy regimen, are “very undervalued by [the] administration.”
“So that stuff feels like it’s faster to get canceled,” he says.
Rowan Martin-Hughes, senior research fellow at the Burnet Institute in Australia, says cutting programs that support prevention and long-term treatment is dangerous.
“With other infectious diseases, you treat people and then they’re recovered; with HIV, people require lifetime treatment,” he told Uncloseted Media. “Most of those people infected with HIV are still alive, and if you take treatment away from them, many people will die. And because treatment is also the best form of preventing transmission, many millions of additional infections will occur.”
Many advocates and lawmakers are pushing back against the cuts. Earlier this month, a federal judge in Boston ruled that the NIH’s DEI-related grant terminations—including many HIV programs—are illegally racist and discriminatory toward LGBTQ people, saying that in his four decades as a judge, he had “never seen a record where racial discrimination was so palpable.” HHS officials say they will consider an appeal.
NIH is far from the only agency issuing massive cuts to HIV. The CDC has terminated large grants to numerous HIV clinics across the country. Los Angeles-based St. John’s Well Child and Family Center lost $746,000, and the LGBT Life Center in Norfolk has lost over $962,000 and could potentially lose a whopping $6.3 million, which makes up 48% of their operating budget. Walls says it’s not just their treatment model that’s taken a hit—the center had to cancel 16 free mobile testing events in June alone, which she fears could cause many more people to contract the virus without knowing, contributing to its spread.
“When we’re out in the community in our mobile testing van, it’s super convenient for people. We’re parked there, they can just walk through, get their test and keep on going, and so that is a low-barrier way to test,” says Walls, who says that easy access is critical for low-income LGBTQ people of color. “[Without it], thousands of people that we test every month or every year are not going to be tested.”
The Vaccine Impact
DEI isn’t the only reason the government has given for HIV-related cuts. The Center for HIV/AIDS Vaccine Development (CHAVD), a consortium of researchers at Scripps Research and Duke University, was informed last month that, after seven years of funding from NIH, their grant would be terminated next year.
Dennis Burton, the program’s director, says they are close to a major breakthrough, with promising technology based on broadly neutralizing antibodies that can disable thousands of different strains of HIV being nearly ready for clinical trials in humans. But without NIH funding, the project may be unable to continue.
“It would put back the development of an HIV vaccine by a decade or longer,” Burton told Uncloseted Media. “We begin to see the light at the end of the tunnel … it’s just the wrong time to stop.”
A senior NIH official told the New York Times that “NIH expects to be shifting its focus toward using currently available approaches to eliminate HIV/AIDS.”
And while Burton says that existing HIV treatment medicine like antiretroviral therapies is “a miracle,” the decision to jettison vaccine research in its favor is misguided.
“The drugs are fantastic … but they’re expensive and people have to take them—the great thing about a good vaccine is that with one or a limited number of shots you can get lifelong prevention,” says Burton. “We want people to live without the fear of HIV, and vaccines are the proven way of preventing viral infections and viral disease.”
The Global Impact
The most sweeping cuts to HIV funding have been to foreign aid. On his first day in office, Trump ordered a 90-day freeze on all foreign aid funding as well as a stop-work order for PEPFAR. While Secretary of State Marco Rubio issued a waiver to continue some critical operations, department memos specifically prohibited funding for PrEP for all populations except pregnant and breastfeeding women.
This move, coupled with the dissolution of USAID and a proposal to cut an additional $1.9 billion from PEPFAR in the FY26 budget request compared to the prior year, has created a perfect storm with staggering results.
The PEPFAR Impact Tracker, a project by Boston University infectious disease modeler Brooke Nichols, estimates that over 60,000 adults and over 6,000 children have died due to PEPFAR-related disruptions between January 24 and June 17. And a survey conducted over the first week of the stop-work order found that 86% of PEPFAR recipient organizations reported that their patients would lose access to HIV treatment within the next month, more than 60% had already laid off staff, and 36% had to shut down their organizations.
The impact hits the hardest in sub-Saharan Africa, the region with the highest HIV concentration, accounting for an estimated 67% of HIV positive individuals globally as of 2021. Numerous long-running and influential LGBTQ health clinics in South Africa have been forced to close, and an investigation by The Independent found that communities in Uganda and Zimbabwe are rapidly being torn apart as more people risk death from lack of access to HIV treatment due to the cuts.
Numerous LGBTQ people told the Daily Sun, a South African digital newspaper, that the closure of long-running clinics like Engage Men’s Health in Johannesburg and Wits Reproductive Health and HIV Institute was devastating.
“I take PrEP, but you can’t go to any clinic as a queer person and ask for it without people looking at you weirdly,” one trans person told the Daily Sun. “At the trans clinic, it was different. Everything was smooth, everything flowed.”
The U.S. has historically been the biggest contributor to fighting HIV, accounting for more than 70% of international funding, but they’re not the only ones making cuts. Following Trump’s example, U.K. Prime Minister Keir Starmer announced 6 billion pounds in funding cuts to foreign aid, including HIV, and France and Germany also announced multi-billion euro cuts.
“HIV has received a lot more funding than any other health area,” says John Stover, vice president for modeling and analysis at Avenir Health. “So it’s a likely target just because the money is so large.”
Martin-Hughes of the Burnet Institute thinks these cuts are dangerous for the entire global health system. He co-authored a study modeling the potential impacts of HIV funding cuts from the major global funders, and the results are grim.
In the worst-case scenario, where PEPFAR is discontinued with no replacement or mitigation alongside the proposed cuts from the top five biggest-spending countries, the study projects that there could be nearly 11 million new infections and nearly 3 million deaths by 2030, which would raise the annual infection rate higher than its 3.3 million peak in 1995.
This is not necessarily the most likely scenario, as PEPFAR is expected to be reinstated in at least some form. However, even the most optimistic estimates show that substantial cuts like the one proposed in the Trump administration’s FY26 budget could still put an end to 15 years of declining infection and death rates—especially since prevention and testing would likely be sacrificed first.
“The world has made really amazing progress on HIV,” Martin-Hughes told Uncloseted Media. “That kind of increase [in infections and death rates would be] a major reversal.” He says that major foreign aid cuts would leave programs for at-risk populations, such as gay and bisexual men, trans women, sex workers and people who inject drugs, particularly vulnerable to being shut down.
Cuts to PEPFAR, a program started by Republican president George W. Bush in 2003, have been controversial even among Republicans, with Senate Appropriations Chair Susan Collins publicly opposing them. While many researchers and policymakers advocate for funding and leadership on HIV to shift away from foreign aid and more towards local governments, Stover and other experts argue that that transition can only be possible with support from PEPFAR in the interim.
“Overall, we all have a vision of more local ownership and control over the resources and how they’re allocated,” Stover says. “[But] it takes time to make this transition, so it’s gonna be practically impossible if funding is just cut off abruptly.”
Cuts on All Sides
Walls says cuts are also happening at the state level. Virginia’s Republican governor Glenn Youngkin slashed hundreds of thousands of dollars for HIV programs, and Walls’ center recently lost multiple corporate donors, including Target, due to pressure from the Trump administration to roll back their DEI efforts.
She says that the fear of backlash for supporting LGBTQ initiatives is so pervasive that even some of their continued donors are now requesting that their contributions remain anonymous.
“Now, if Target was to advertise that they were giving money to the LGBTQ community center in their neighborhood or city, they would have consequences from the administration or even shoppers,” she says. “They’re not gonna take that risk.”
Meanwhile, Walls says the LGBT Life Center is staying afloat thanks to the local community stepping up, with an unprecedented number of people signing up to be volunteers and local restaurants and other businesses providing their assistance, whether that’s by participating in citywide fundraising events or offering to help paint the clinic.
“It is amazing to see, and I know that through all of this the community will help carry us through, because we have brought value to this community for 36 years and I feel confident that people see value in our services,” she says.
Still, experts, advocates and infectious disease modelers agree if HIV funding doesn’t continue, the effects will be devastating.
"I think it's hard for people to look at these numbers and not feel like it's important to prioritize," says Martin-Hughes. "There needs to be, to avert these worst-case scenarios, sufficient funding for those programs."
If objective, nonpartisan, rigorous, LGBTQ-focused journalism is important to you, please consider making a tax-deductible donation through our fiscal sponsor, Resource Impact, by clicking this button:

Obtained via data from Grant Watch 06/17/2025. Sum of terminated funds for all grants where HIV was listed under “terms.”